

Philly region’s COVID cases were 7 times higher than originally recorded, CDC finds
A study released Monday examined the results of antibody tests conducted in 10 geographic areas around the U.S., including the Philadelphia metro region.

Blood collection tubes sit in a rack on the first day of a free COVID-19 antibody testing event at the Volusia County Fairgrounds in DeLand, Fla., on May 4<strong>.</strong> (Paul Hennessy/Echoes WIre/Barcroft Media via Getty Images)
Updated: 1:08 p.m. Thursday
___
On Saturday, April 25, Pennsylvania Health Secretary Dr. Rachel Levine stepped to the podium to address the media at her daily coronavirus press briefing.
With a cloth face-covering hanging limply around her neck, she read through the grave data points just as she did every day. By this point, there was a bit of hope: the number of new COVID-19 cases had begun to fall, signaling that the deaths would too, soon. It appeared as if the worst was behind us.
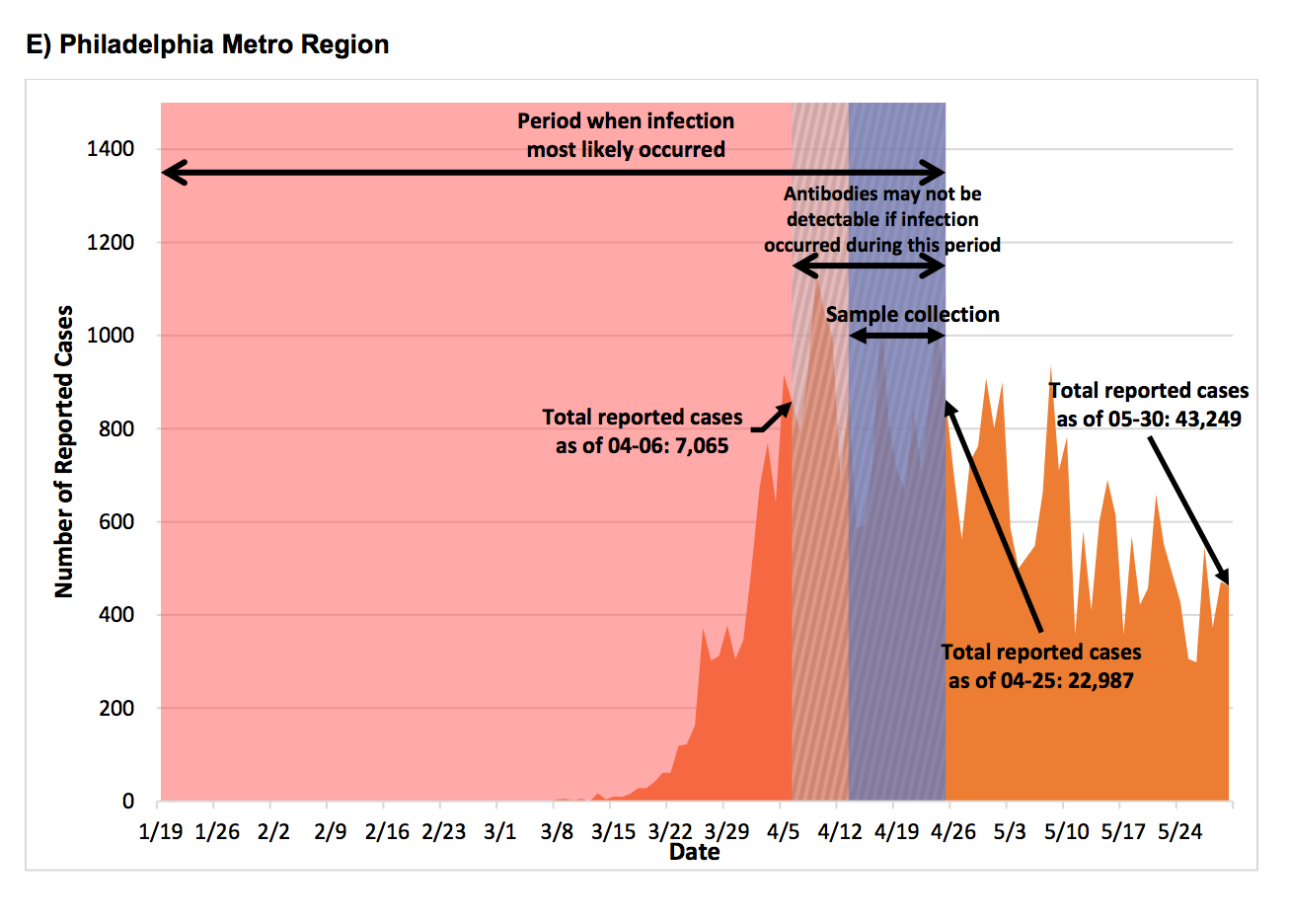
But while the case numbers may have been on the decline, new research suggests that the reported number of SARS-Cov-2 cases was, in fact, a dramatic undercount. The virus was circulating in the community at a rate seven times greater than that detected by the state.
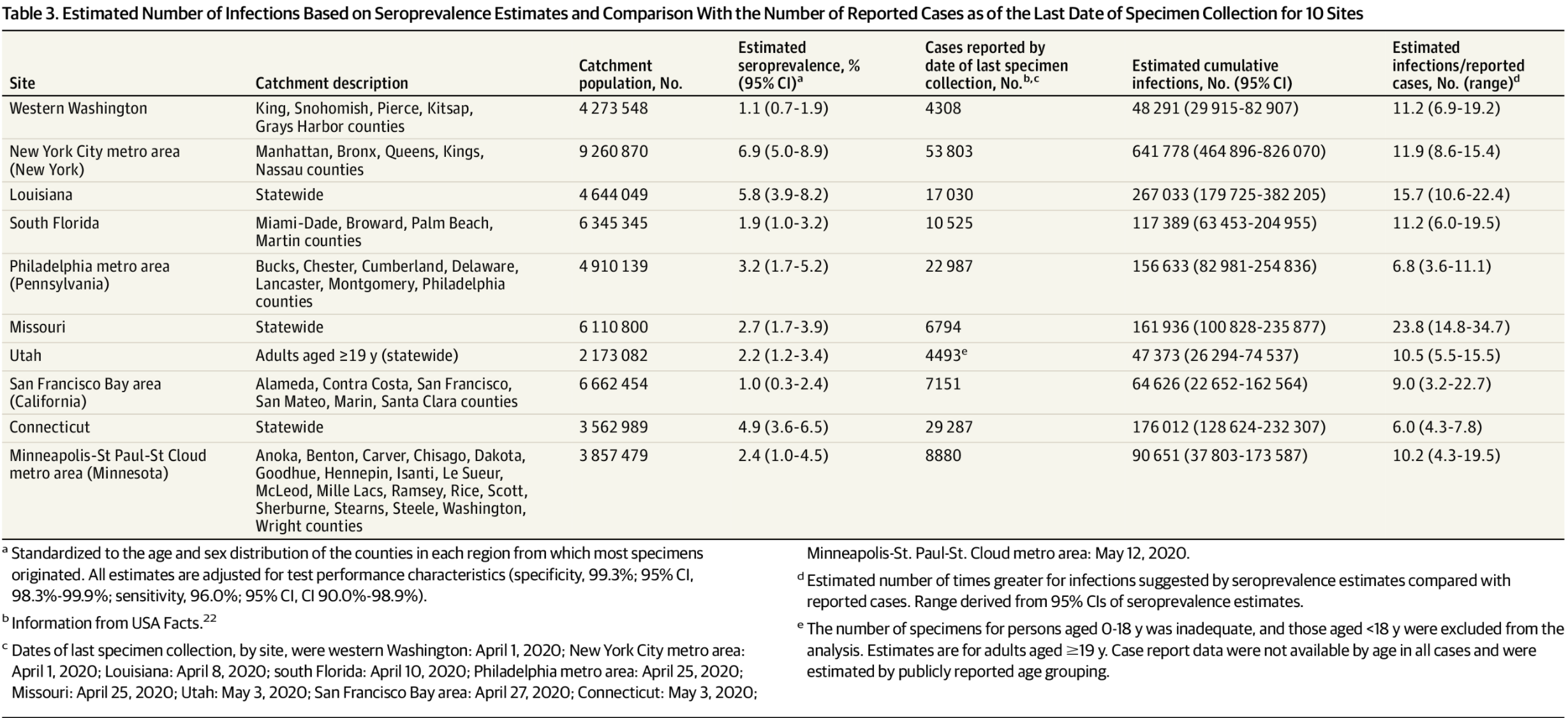
The study, released Monday in JAMA Internal Medicine, examined the results of antibody tests conducted in 10 geographic areas around the country, including the Philadelphia metro region. On April 25, the number of documented COVID-19 infections had reached nearly 23,000 in Philadelphia and its surrounding counties, Bucks, Montgomery, Delaware and Chester — as well as in Cumberland and Lancaster counties, which the agency included. To determine how many more people had contracted the virus without receiving diagnostic tests in the months leading up to that date, researchers collected serological samples from people at routine medical appointments for 12 days prior. They found that the actual number of cases was 156,633 — seven times greater than the number of tests recorded.
The serological samples were taken from patients who were already seeking medical attention for something, so they were not entirely random and could have had more potential exposure to the virus than others in the population.
“Data collection periods overlapped with active stay-at-home orders, when most medical appointments and elective admissions were deferred,” wrote Drs. Tyler S. Brown and Rochelle P. Walensky, both with Massachusetts General Hospital, who co-authored a companion editorial to the study, which included researchers from the Centers for Disease Control and Prevention. “Thus, the outpatient and inpatient populations included in the study are likely not representative of a typical pre-pandemic cohort; some of the discarded serum specimens from inpatients were likely obtained from patients hospitalized for COVID-19.”
The CDC is expected to release two random studies focused on Indiana and Georgia in the coming days.
Related Content

Philly mulls later start time for high schoolers amid pandemic planning
The coronavirus could prompt a radical change for when Philly teens start school. Will that lead to better-rested students? Or upend family routines?
6 years ago
There are a number of explanations for why so many cases were missed.
Due to the initial nationwide testing shortage, anyone experiencing moderate COVID-19 symptoms who was otherwise healthy was instructed to stay home and self-quarantine but not seek testing. That way, what limited supplies were available could be conserved for the elderly, those with underlying conditions, and health care workers. That instruction alone could account for thousands of symptomatic cases that went undetected.
“This testing capacity is now much improved, largely due to the assistance in receiving test supplies from the federal government,” Health Department spokesperson Nate Wardle wrote in an email. “Now, if you need to be tested, there is testing available. We encourage any Pennsylvanian who is experiencing symptoms or came in contact with a COVID-19-positive individual to get tested.”
But more tests won’t catch those without any symptoms who are still able to spread the virus, therefore contributing to its transmission throughout the community. About 40% of those with COVID-19 are thought to be asymptomatic. To accurately count asymptomatic carriers would require random testing; to prevent them from spreading the virus would require ongoing precautions like mask-wearing.
Compared to the other areas analyzed in the study, the Philadelphia region fared rather well. The researchers estimated New York City had 12 times the number of recorded cases based on antibodies, and the true count across the state of Missouri was likely 23 times greater. Of the areas studied, only the state of Connecticut had a lower margin than Philadelphia, where the actual number of cases was six times greater than those documented.
The overall rate of people with antibodies in this region was just over 3% of the total population — nowhere near the 60% to 70% threshold needed for herd immunity, in which enough of the population has contracted the virus that transmission rates decrease. Plus, researchers are still determining the impact that antibodies have on strength and length of immunity.
How might the response to the virus have been different if the true number of cases was clear in real-time?
Gov. Tom Wolf used a variety of metrics to guide the reopening of economies in each county. Those included overall case counts, testing capacity, robust contact tracing, and case investigation infrastructure and hospital capacity. Many have criticized Wolf for allowing counties to begin reopening before they satisfied those benchmarks. The counties would have certainly fallen short if the true number of cases was reflected.
Wardle said that “probable cases” — including positive cases resulting from antibody tests — “were not used for the decision-making process of moving counties into the reopening process across Pennsylvania.”
The state has recorded only 637 “probable cases” resulting from antibody tests since April 12. The fact that the study recorded tens of thousands of people with antibodies, while just hundreds of those who sought antibody testing received positive results, perplexes Pennsylvania Health Department officials.
“It does raise the question as to why the data has not been reported to us,” Wardle said in the email, referring to the serological lab results reported to the CDC.
Going forward, Brown and Walensky contend that the study’s findings should make governments think twice about how much testing they need to keep the virus in check.
“Large differences between known, reported cases and the serology-based estimates reported … underscore how limited [diagnostic] testing capacity, including both the massive shortfalls that derailed the early epidemic response and the ongoing lack of testing for active surveillance, have left enormous numbers of infections undetected, circulating in the community, and propagating the epidemic,” they wrote.
In one sense, the report offers some good news: The retroactively identified cases are likely to have been less severe — or in many cases, symptomless — since they didn’t require hospitalization.
That might demonstrate that the death rate of the virus is lower than originally estimated since more people had contracted it without dying. Although that, of course, does nothing to change the total number of lives lost.
___
This article was updated to include comments from the Pennsylvania Department of Health’s spokesperson.
Get daily updates from WHYY News!
WHYY is your source for fact-based, in-depth journalism and information. As a nonprofit organization, we rely on financial support from readers like you. Please give today.
Part of the series


Amid CDC turmoil, Pennsylvania joins Northeastern states in regional public health coalition
The Northeast Public Health Collaborative has formed working groups to identify opportunities for states to share emergency public health planning and response resources.
10 months ago

Rethinking advice amid COVID summer surge: How long do you really need to isolate?
If you Google COVID isolation standards, you're likely to get a few different answers. So which one should you follow?
2 years ago
Listen 1:09
Philly, several suburban counties now seeing substantial COVID-19 transmission
Days after the CDC issued new masking guidance for fully vaccinated people, much of the Philadelphia region is experiencing “substantial” levels of COVID-19 transmission.
5 years ago
