

Medicare and the desegregation of health care
It wasn’t that long ago that separate hospitals for black and white patients were the norm in America, but then all of that changed — and it changed quickly.
Listen 13:20
A segregated obstetrics ward at University Hospital,University of Alabama, Birmingham. (Courtesy of UAB)
It wasn’t that long ago in America that separate hospitals for black and white patients were the norm.
In places where a black hospital didn’t exist, black patients might not have anywhere to go for emergency care. Or, they’d be directed to separate entrances, waiting areas, and wings of a hospital. But then all of that changed, surprisingly quickly, when Medicare took effect in 1966. Historian David Smith says there were “magic months” leading up to that time.
Refused care
Brenda Armstrong grew up in Rocky Mount, a rural town in North Carolina. The daughter of a doctor, she remembers how black patients were treated unequally in hospitals.
“They waited a longer time in the E.R. to be seen. They were addressed in demeaning ways,” Armstrong said.
Armstrong is 69 and an outspoken doctor now, but when she was just a little girl she had an experience that she could not shake, which would fuel her passion and her lifelong work. Her mom was pregnant with her baby brother. Her dad, who was a doctor, knew that mom and the baby were in danger, that mom needed a C-section. She was a petite woman, and the baby was big. Armstrong recalls her dad reached out to the hospital in town that could handle the situation, but that hospital was for whites only.
“So my dad, he was a very proud man, and he asked if they would make exception,” Armstrong said. “And they said no.”
In 1956, Brenda’s baby brother was born, at home, without a C-section.
“I remember my dad coming to pick me up at school to tell me what had happened. It was difficult,” Armstrong recalls, tearing up when she thinks about it. “I thought he was going to tell me that my mom had died.”
Actually Armstrong’s mom was just a little sick
“But my brother was in trouble. And we just didn’t know what was going to happen.”
Her brother had had a stroke that left one side of his body permanently damaged. That stroke, she says, probably could have been prevented had her mother not been turned away from the nearby local hospital, the white one.
“I was angry, I still am,” Armstrong said.
A turning point
This denial of care was standard practice back then, but by the ’50s, a movement was growing to challenge the status quo, to fight back against the segregation.
From restaurant sit-ins to bus boycotts, the civil rights movement was gaining momentum. And in Greensboro, North Carolina, a group of black doctors and patients set the foundation for the changes in health care.
Gwen Blount Adolph is the daughter of one of those doctors, Alvin Blount. “I know that one of the things that just bothered my dad and his peers was they could not treat patients in the hospital that had the better facilities,” Blount said.
Those were the facilities only for white people.
“It wasn’t about the better quality of doctors, but it was about equal access to quality facilities,” she said.
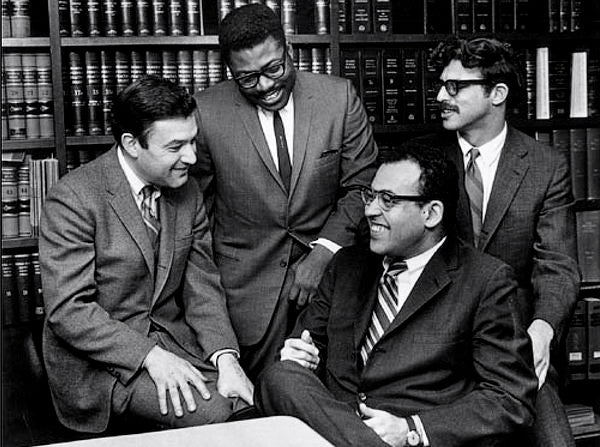
Blount’s colleague, George Simkins, kickstarted their efforts. He was a prominent activist and dentist. When one of his patients needed to be hospitalized for an abscessed molar and was refused care at the white hospital, they’d had enough. Simkins organized everyone and reached out to the Legal Defense Fund. The fund often operated as the legal arm of the civil rights movement. Michael Meltsner took up their complaint.
“I was the one lawyer at the Legal Defense Fund who handled health cases,” Meltsner recalled.
They composed a plan. Simkins, Bluont, and others applied for staff privileges at the white hospital.
“They were of course refused and rejected. In one case they didn’t even get a response. And so on that basis we filed a complaint,” said Meltsner, who has since written about the experience.
They challenged the federal status quo and more specifically, a post WWII law — the Hill-Burton Act — that actually allowed hospitals to get federal funding, even if they were for whites only.
The case went through the legal wringer, but it came on the heels of the landmark Brown v. Board of Education ruling that overturned the notion that separate was equal in public schools. The black doctors from Greensboro essentially argued the same thing for publicly funded hospitals. They won when the Supreme Court refused to take up an appeal to a lower court decision.
The principle that separate is unequal was then adopted into Title VI of the Civil Rights Act. It clarified plain and simple that hospitals could not discriminate if they wanted federal money.
“Which on the face of it should have ended the racial policies of about 6,000 southern health facilities, hospitals, clinics and the like,” Meltsner said.
“But really almost nothing happened,” he said.
The ‘gift’ of Medicare
At that time, hospitals didn’t rely heavily on federal money. And without any major penalties, they didn’t have a big motivation to change, to let black patients or doctors through their doors. Meltsner said lawyers would have had to take each and every health facility that continued to segregate to court, and that would require resources they didn’t have.
In 1965, the landscape radically changed, when “along came a gift,” Meltsner said.
Medicare was the gift.
President Johnson signed the massive health legislation into law on July 30, 1965.
Medicare was the new health care program that would cover seniors and Americans with disabilities. Under the program, the government would now generously pay for the care of millions of people.
This new-found health care funding had the potential to change everything, to tear down hospital segregation. But that would require more than just a rule on the books. A tiny government unit took on the responsibility.
Some say it was a David vs. Goliath fight.
Peter Libassi led that unit, inside the Department of Health Education and Welfare, or HEW. Today he lives in a a retirement home in Connecticut. He says a little civil rights unit of just six people was tasked with creating and enforcing the rules that hospitals would need to follow to be eligible for the lucrative new medicare funds.
“I’m talking about 25 percent of their income they were hoping to get from hew that year,” Libassi said.
The core rule was that no hospital would get any funding until they were completely integrated. No ifs, ands, or buts.
Early on, Libassi remembers reporting the pushback to one of the higher ups in his office.
“He said, ‘Pete! Tell me what’s up how’re you doing?’ I said, ‘Doing fine, Joe!’ He said, ‘What do you mean?’ I said, ‘You should know that there isn’t a hospital in the South that’s desegregated, so no one will be eligible for the money.’ He said, ‘What did you say? Are you out of your mind?!’”
But the government got behind Libassi’s efforts. It was a game changer.
The tiny enforcement teams
“So, when the federal government decides to act and there’s urgency about it, gosh it’s fantastic,” Libassi said. “People around the country began to organize visitation teams.”
Peter’s unit, remember, was small, just six people. They needed help. And help they got. People from all over the government stepped up — doctors from the public health service, bench scientists, men and woman, black and white — who wanted to see these changes in health care through.
Libassi says they were divided into teams of three, made up of someone who specialized in medicine, a government worker from the local community, and someone who knew the law. These teams went out to investigate the hospitals, often in person and on the ground, to ensure that hospitals wouldn’t get any money, not a dime, until they were actually fully integrated.
“This was going to require 18-hour days, threats on their lives,” said David Smith, a Drexel University professor who has written a book about this effort and has interviewed some of those team members. “They would be chased by the klan, their windshields would be shot out, crosses would be burned on their lawns, and most of the people who volunteered knew.”
Smith says everybody had a story. There was a black doctor who went in as part of a three-person team to Marshall County, Texas, to see if he could put pressure on the local hospital.
“The administrator told him to go to hell, that they would never integrate. So the physician said “Ok, but you just lost $5 million in funding for next year for your hospital,’” Smith said. “Three days later, that physician is called by the chair of the [hospital] board who says, ‘We just fired the administrator. Tell us what we have to do to get the money!’”
Sometimes hospitals would try to cheat and fool the teams, Libassi recalled.
“It was ridiculous. But the teams would say, ‘Wait a minute! This is not desegregation when you put one black person in one bed up here, you need to desegregate the whole hospital, don’t you understand? The whole place has to be desegregated or you’re going to get the money,’” he said.
Local constituents complained, word got up to their congressmen. And so while those teams were on the ground, Libassi spent a lot of his time testifying and defending their efforts in Washington, D.C.
At the same time, Smith says hospitals who did make the shift tried to do it without much visible fanfare.
“Nobody knew anything about this, it was kept very quiet,” he said. “Hospitals didn’t want to make a big deal about this because they were afraid the local community would be up in arms. They were very quiet about it.”

Changes set in
Within a few months, the teams had more or less succeeded: 98 percent of hospitals had integrated.
In July of 1966, one year after medicare passed, the program was ready to go, the money was ready to flow.
“So my grandmother was one of the first people to get a Medicare card, because you could apply for it in January if you had already passed your 65th birthday,” said Edith Mitchell, M.D. She’s a professor of medical oncology at the Sidney Kimmel Cancer Center at Thomas Jefferson University.
Mitchell grew up in Brownsville, Tennessee, and she witnessed this transition when her grandmother needed help.
“She got admitted to the hospital,” Mitchell recalled.
Her grandmother was 65, and she had never been to a hospital before. It was a good experience.
A few years later, Mitchell was on her way to becoming a doctor herself. She’s also a researcher now, leading efforts to reduce racial disparities in cancer. But as a young med student in Virginia, she got to see the changes from the inside.
“Nursing staff integrated, so they could work on any ward. Black doctors were given medical privileges, so that they could admit and take care of their patients in those hospitals,” Mitchell said. “It was just amazing.”
She says in the years right after Medicare took effect, fewer black babies died. Health improved. Racial inequities narrowed.
Back in North Carolina, another up and coming doctor was taking in the transformation.
“It wasn’t until I came back to Duke in the ’70s to do my residency and fellowship training that I could tell a big change,” said Brenda Armstrong, whose baby brother had experienced a stroke that was likely preventable when he was born, because he was refused care at the local, whites-only hospital.
Armstrong kept that experience close to her heart. She became a pediatric cardiologist, and a dean at Duke’s medical school.
“Being dean of admissions of the medical school gave me a chance to challenge Duke to do the right thing,” Armstrong said.
When Brenda first started out decades ago, she says too many really smart and qualified African-American students got turned away. That’s been changing.
“Duke has done better than almost everyone in the country in the recruitment of women, of students of color,” she said.
Now black students make up nearly one-fifth of the med school.
WHYY is your source for fact-based, in-depth journalism and information. As a nonprofit organization, we rely on financial support from readers like you. Please give today.
Brought to you by The Pulse


Finding our family’s roots through the ‘sepia rainbow’
Genealogy often looks like thumbing through old documents and pictures, but what story does skin color tell about family lineage?
2 years ago
Listen 1:51
A biased test kept thousands of Black people from getting a kidney transplant. It’s finally changing
The U.S. transplant system ordered hospitals to quit using a test that made Black patients' kidneys appear healthier than they really were.
2 years ago

How informal adoptions became a mainstay of African American family life
This story is from The Pulse, a weekly health and scie ...
5 years ago
Listen 9:47