

‘Without data, there’s no equity’: Deficient Asian American COVID-19 data masked community-wide disparities
Asian Americans were most likely to be misclassified in coronavirus statistics, despite a disproportionate burden of infection and mortality.

Community health workers and field staff assisting with food delivery during the COVID-19 pandemic in New York City's South Asian community. (Courtesy of Nadia Islam)
Ask us about COVID-19: What questions do you have about the coronavirus and vaccines?
At the outset of the pandemic, New York City was the first region in the country to experience widespread COVID-19 contraction and death rates, with more than 200,000 cases, 50,000 hospitalizations, and 17,000 deaths between March 1 and May 31, 2020. As state, city, and federal data, including statistics from the Centers for Disease Control and Prevention were released, uniquely high burdens of infection among the city’s and the nation’s Black and Latino Americans were reported, with Asian Americans reported as experiencing only a slightly higher burden than white Americans.

But Nadia Islam says a whole different story was unfolding on the ground before her, a story the data completely masked.
“What was really stunning to us was that so much data was coming out from places like New York City with missing race and ethnicity data,” said Islam, who is an associate professor in the Department of Population Health at NYU’s School of Medicine. “And that missing race and ethnicity problem is a particular problem for Asian American communities because we tend to be misclassified or counted as ‘other’ more often than other groups.”
New York City is home to the second-largest Asian American population in the country, and Islam said data issues there are most likely reflective of issues across the country as well.
Islam oversees the Diabetes Research, Education and Action for Minorities Initiative, a community health worker intervention that addresses the burden of cardiovascular disease in New York City’s Bangladeshi community.
Community health workers serve as a bridge between communities and health care systems and help move the needle on long-standing health disparities doctors and clinicians have trouble addressing. Unlike other kinds of health care professionals, community health workers share life experience with the people they serve and often have leadership roles within the community so they can leverage trust in unique ways.
According to Islam, South Asians in New York City compose a large part of the essential workforce, with high concentrations in low-wage, service sector jobs such as taxi driving, restaurant work, and managing grocery stores. These types of jobs have a serious impact on their health outcomes.
“If you think about a taxi driver who has a 12-hour shift, it’s a very sedentary job,” said Islam. “They need to think about where they can park their car to be able to take breaks. So they’re often eating on the job, [with] very little opportunities for physical activity.”

By mid-March 2020, Islam said, her community health workers were hearing countless reports about people losing jobs and fears of not being able to find work. As the community health workers pivoted to food and medication delivery during the early days of the pandemic, they became overwhelmed by reports of COVID-19 infection and deaths from the families and individuals they served.
“Within two weeks, it was devastating to me how quickly it happened,” recalled Islam. “It was like an avalanche of death and dying.”
Related Content

Vaccine clinic for Philly immigrant communities helps bridge gaps in COVID-19 care
Friday was the first of three scheduled first-dose opportunities to take place in Center City. All vaccinations are by appointment.
5 years ago
Asian American data more likely to be missing or misclassified
In April 2020, Islam and her community health worker team conducted a COVID-19 needs assessment of New York City’s South Asian communities. Of the 200 people they reached and surveyed, she said, close to 40% knew a close friend or family member who had died from the virus.
Stella Yi, an assistant professor at NYU’s Grossman School of Medicine, said New York City’s Health Department released race-specific data on April 8, 2020. But it just wasn’t adding up with the community-level reports from throughout the city, she said.

“The [Health Department] number was close to 112 deaths,” said Yi. From Islam’s community health workers, “we literally had heard [on April 7] that it’s 85 in the Bangladeshi community alone. And now you’re telling me that it’s 112 [Asian American deaths] total for the whole city? No way.”
Yi said accurate collection of race and ethnicity data has been lacking for Asian Americans and other communities of color for some time, and has been especially pronounced during the pandemic. And, according to Islam, the real problem stems from the fact that “Asian American” as a term is an umbrella category, representing 30 different subgroups from a variety of ethnic backgrounds and languages. But data that is reported on Asian Americans is often aggregated, which essentially makes it meaningless, Islam said.
“There is such tremendous diversity in the population that comparing a Chinese person to a Hmong person is — there are very few real similarities there, and the experiences are very different,” said Islam.
In addition, there is a significant bimodal distribution in the Asian American community in terms of socioeconomic characteristics. That means that while there is a proportion of the Asian American population that’s very high-income, but there’s also a very low-income, immigrant group with limited English proficiency and educational attainment. Aggregated data erases those distinctions.
Yi added that there’s also a more sociological question about who counts as Asian American. She cited the research of sociologist Jennfer Lee, which found that “East Asians describe themselves as being Asian American. South Asians describe themselves as Asian American. But white and Black [people] and East Asians do not ascribe South Asians as being Asian American,” she said.
When Asian American data collection isn’t conducted by Asian Americans, Yi said it’s more likely that race and ethnic markers won’t be marked down at all.
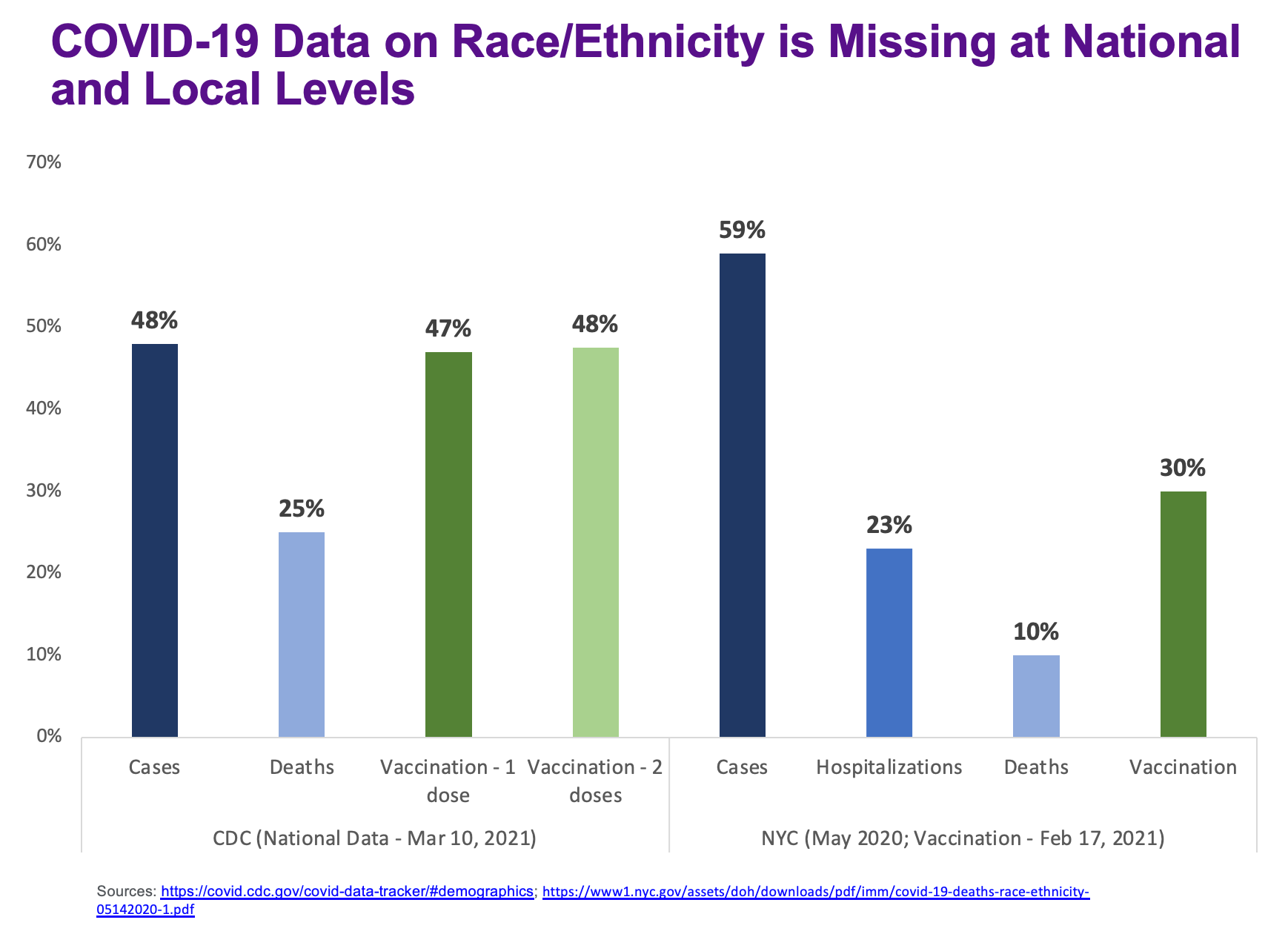
“If you see someone with darker skin and it’s ambiguous what they are, then they’re probably put in as ‘other’ or ‘missing’ or ‘unknown,’” said Yi. “If you look at the Health department data from April 8 … race and ethnicity is missing for [almost] 60% of cases, 10% of deaths, and 20% of hospitalizations. So there’s a huge amount of misclassification.”
Poor health data masked COVID disparities in the community
Roopa Kalyanaraman Marcello is the Senior Director of Research and Evaluation at NYC’s Health and Hospitals Corporation. Though CDC data has continued to show Asian Americans experiencing only a slightly higher burden of COVID-19 infection and deaths than white Americans, a 2020 analysis led by Marcello of 85,000 patients tested for COVID-19 in New York City’s public hospital system — the largest such system in the country — between March 1 and May 31, 2020, showed that South Asians had the second-highest infection and hospitalization rates for COVID-19, second only to Hispanic Americans. And Chinese Americans had the highest COVID-19 mortality rates compared to all other racial and ethnic groups.
Kalyanaraman Marcello, Yi, Islam, and other colleagues used pre-existing race and ethnicity data from the hospital system and conducted what they call surname analysis to correctly classify and reclassify Asian American patients in the data pool. In 2000, researcher Diane Lauderdale worked with a team to create a system that used common surnames from the 2000 Census to classify people into six of the largest Asian subgroups.
“So we used the Lauderdale list, and then [Islam] had a list she had gathered from her study participants and community members — names that would be newer and would not show up in the Lauderdale list,” said Yi.
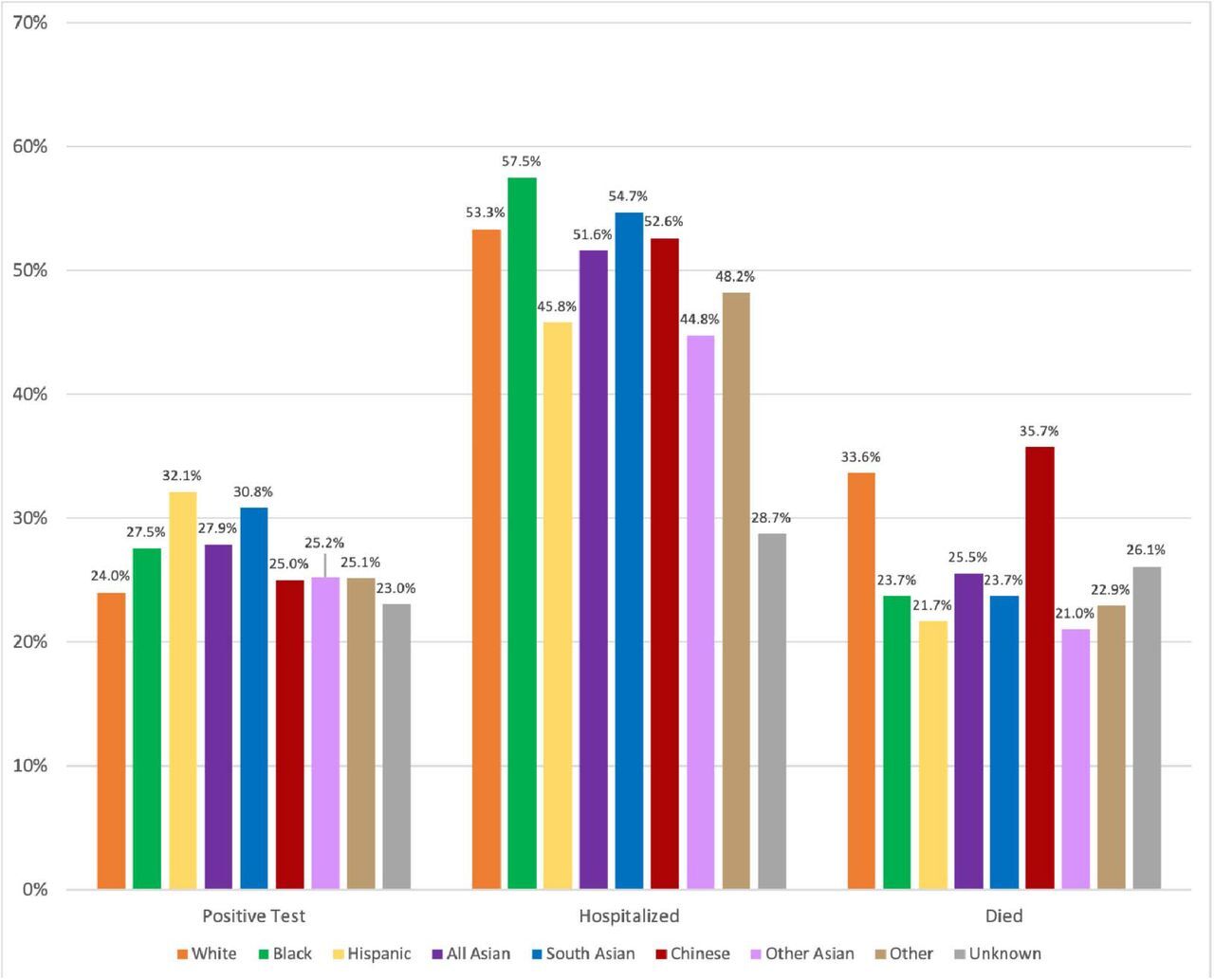
One of the central points of the analysis, Yi said, is that aggregated Asian American health data showed lower rates of positivity, hospitalization, and mortality when compared to other ethnic groups. But when they looked at specific Asian subgroups, the COVID-19 disparities were clear as day.
Risk factors such as diabetes, hypertension, and cardiovascular disease were common among Chinese and South Asian patients, conditions that are known to elevate the risk of COVID-19 overall. Yi believes social factors like increased xenophobia discouraged Chinese patients specifically from seeking out care until they were quite sick from the coronavirus.
“And also I think there’s kind of a lack of attention placed on preventative care,” said Yi. “It’s like you only go in if you’re really falling down and broken.”
But accessing preventative care isn’t always possible among Asian American immigrants in New York, who may delay care due to immigration concerns. For frontline workers, lack of paid sick leave, as well as lack of access to COVID-19 information in their first language, contributed to the disparities.
“Another thing that we saw early on [in the pandemic] is that not all communities were reached equally in terms of information dissemination, and that that is ripe and fertile ground for misinformation at the community level,” said Islam. “And so we definitely saw the impact of that in the South Asian population.”
Asian Americans are also more likely to live in multigenerational housing. If you’re an essential worker who cares for your 80-year-old grandmother at home, there’s not much you can do to physically distance from her and limit your own exposure to the virus outside the home.
Related Content

This special workforce is alleviating COVID vaccine fears in the most vulnerable communities
Community health workers get to know clients personally by asking them what they need to improve their health, and they raise vaccine trust in hardest-hit groups.
5 years ago
Listen 6:11Good data: the cornerstone of an effective response
As COVID-specific grants and funding started to roll out from the federal government and state and city-level agencies, Yi said she felt an urgency to collect Asian American health data quickly and accurately. If you can’t prove there’s a disparity within a community, then you can’t receive and disseminate funding to that community in need.
“Without data, there’s no equity,” said Yi. “And if there’s not data then there’s no disparity. When Asian Americans were being left out of the conversation, people just assume that there’s no disparity. But usually it’s because there’s no data.”

Now, Yi said, she and a team at NYU are studying and developing ways to more accurately capture race and ethnicity data across many groups. She said that misuse of race in medical practice has been an ongoing issue, and that it’s particularly pronounced in New York City, where immigrants make up 38% of the city’s population and 45% of the workforce.
“It doesn’t matter if you’re from Kenya or Jamaica, you get categorized as Black,” said Yi. “But in New York, one of the largest immigrant communities here is the Carribean Black community. So it’s not adequate anymore to [ask for] race and ethnicity. We have to be thinking about country of origin.”
Dr. Jaya Aysola is an assistant professor of pediatrics at the University of Pennsylvania’s Perelman School of Medicine and executive director of Penn Medicine’s Center for Health Equity Advancement. She and her team focus on bringing the science of equity to daily health care operations.
“Race is not a meaningful scientific construct, it’s a social category that reflects the impact of unequal social experiences in health,” Aysola wrote in a study co-written with colleagues in the New England Journal of Medicine that analyzed 880 lectures from 21 courses in one institution’s 18-month preclinical medical curriculum. The study found five key domains in which medical school educators misrepresent race in their interpretations of race-based data.
While race and ethnicity refer to social groupings that are based on some combination of shared language, culture, history, or religion, Aysola said, they are both poor proxies for ancestry, family history, and country of origin, which are better indicators for predisposition of diseases.
‘The fundamental problem has been lack of political will’
Islam’s community health workers helped uncover the gaps in South Asian health data in the early months of the pandemic. That’s not by accident, she said: The community health worker model isn’t just about targeting specific burdens of disease. It encourages health workers to take in the whole of a person, and meet them where they are at.
The community health workers didn’t set out with the sole purpose of collecting data. When disseminating food and medical supplies, they spent time listening to their South Asian clients, who were feeling especially isolated by social distancing and needed that listening ear. During these conversations, they shared stories of COVID-related deaths and infections.
“It’s not just asking the questions and getting the responses, it’s hearing the whole story,” said Islam. “They would assess the need, and then our [community health workers] would link someone to unemployment resources or help set up food delivery, so it wasn’t just data collection without follow-up.”
Yi and Islam said there’s a critical need for quality health data across racial groups. But for Asian Americans in particular, dominant perceptions are limiting that work.
“I think the fundamental problem has been lack of political will,” said Islam. “There is just a very stubborn perception of Asian Americans as both a model minority and a perpetual foreigner that I think [is] sort of underpinning [the idea that] we are a ‘small’ population.”
“Asian Americans are 5% of the population nationally, but 15% in places like New York City. They’re projected to be 10% of the population by 2050. So I think the small population argument is just simply not relevant anymore.”
—
Support for WHYY’s coverage on health equity issues comes from the Commonwealth Fund.
Get daily updates from WHYY News!
WHYY is your source for fact-based, in-depth journalism and information. As a nonprofit organization, we rely on financial support from readers like you. Please give today.
Part of the series


COVID-19 supplies and other public health services at four resource hubs will move to new community action centers at different city locations.
1 month ago
Listen 1:17
Racial health gaps persist in Pa., N.J. and Del. as Medicaid cuts loom, report finds
The Commonwealth Fund’s 2026 State Health Disparities Report showed health care gaps were the greatest among Hispanic residents.
3 months ago
Listen 1:13
5 years since the pandemic started, long COVID patients are still hoping for a cure
They're pushing for more funding to find effective treatments. Researchers are finally starting to make headway but have a way to go.
1 year ago
